
Known Crohn's disease and how to deal
Written by:Crohn's disease is an inflammatory bowel disease. It can affect any part of the digestive system, causing ulcers. Depending on the symptoms presented by the patient and disease progression medical treatment, surgery, or both shall be indicated.
Crohn 's disease: what it is and what causes it
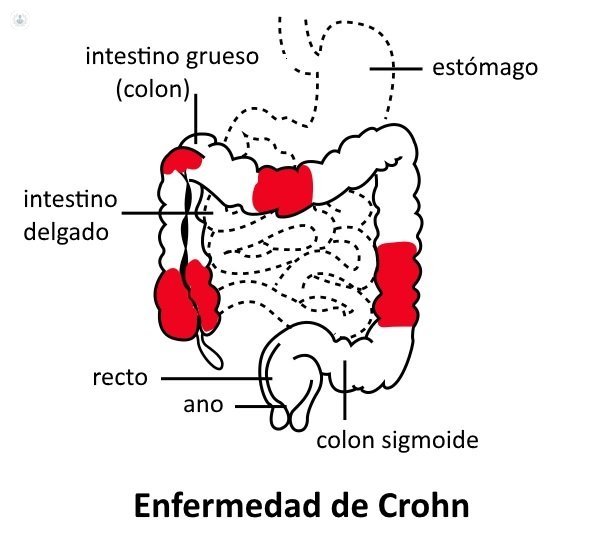
It is a chronic inflammatory bowel disease that can affect any part of the digestive tract, from the mouth to the anus, causing multiple small ulcers that can pass through the entire thickness of the intestinal wall. These are the most important differences with other inflammatory disease, ulcerative colitis, although in some cases may be difficult to distinguish. It produces very significant healthcare costs.
It is not known why this disease occurs, although it may be triggered by the combination of several factors, including genetic in about 20%, and also the immune system (body defense), bacteria (flora or intestinal microbiota ), or food.
Prevalence of Crohn's disease and risk factors
Crohn's disease occurs most often in young adults and is more common in developed countries. In addition, it continues to increase significantly. The known risk factor on which we can act is the snuff. Smokers have a higher risk of developing the disease and have more inflammatory outbreaks and more serious.
Symptoms and diagnosis of Crohn's disease
Crohn's disease can cause abdominal pain, fever, diarrhea or fistula formation, among other symptoms. Sometimes there is also other organs such as inflammation of the joints, skin or eyes.
It develops in crisis or inflammatory outbreaks more or less severe with periods of stability between them and can cause abnormal communications between the gut and skin, or between different parts of the intestine (fistula), accumulation of pus (abscess) and strictures that impede the passage of intestinal contents (stenosis). The most commonly affected part of the intestine is the end of the small intestine (ileum) and the beginning of the colon (cecum), followed by colon and rectum, but may appear in other sections, or several simultaneously. Sometimes affects the anus and can cause discharge from fistulas, which can be complex, pain or bleeding. Suspecting Crohn's disease diagnosis can be performed by endoscopy (colonoscopy or capsule endoscopy), intestinal radiologic studies or, more recently, magnetic resonance intestinal (Whole-resonance) as well as different types of analysis in blood and feces.
Treatment of Crohn's disease
The initial treatment of Crohn's disease is a doctor. The disease can not be cured but can be relieved significantly and not even present outbreaks for years. It includes the use of anti-inflammatory drugs and corticosteroids or 5-ASA (mesalazine) and sometimes antibiotics. Corticosteroids have many side effects and, therefore, try to reduce or eliminate where possible.
Major outbreaks of disease require hospitalization and sometimes using special medications like immunosuppressants, called biologics, or artificial nutrition to let stand the intestine. It requires collaboration between different specialists, including colorectal surgeons , the correct orientation for treatment of patients.
When surgery is required for Crohn's disease
It requires at least surgery between 50 and 70% of patients and this may be indicated emergency to serious complications such as bleeding, obstruction or perforation of the bowel, but much more frequently in those with a chronic form of the disease failure of medical treatment, complications, frequent or severe outbreaks, or serious side effects from the use of medications.
Other indications are the existence or suspected cancer or nutritional disorders. In addition, they often need surgery for anal problems, mainly abscesses or fistulas. Surgery is the last resort in the treatment of this disease and should be set by consensus by the gastroenterologist and the surgeon who treated the patient.
What they are surgeries for Crohn's disease
Surgeries for Crohn's disease often require removal of the portion or portions causing intestinal problem. Although less aggressive should be possible in this disease, and you have to remove the minimum necessary intestine and often with the use of laparoscopic surgery, when there are serious effects fistulas or surgery can mean a technical challenge that requires a colorectal surgeon with experience.
At other times, when there are only small cause strictures of symptoms, we can widen without removing intestine (plasty). Since the surgery is not curative and may be involved a patient throughout his life on several occasions, interested preserve as much as possible to avoid future nutritional bowel problems. It is possible that the patient requires carrying a stoma (bag to evacuate) at some time, temporarily or permanently.
When there is involvement of the year it is required sometimes empty accumulation of pus (abscess) and place small drains piercings similar to rubber, to avoid discomfort and complications. Sometimes you have to try anal strictures, fissures, and more frequently, skin fistulas or neighboring organs such as the vagina in women.
Postoperative Crohn's disease
Postoperative Crohn's disease is variable depending on the type of intervention, its complexity and the previous state of the patient (medication, nutrition). The, although rare, major complications are intestinal suture failure or fistulae. But in general, and since the disease affects young patients, recovery is good, and corrected the problems indicated the surgery, the patient improves their status and quality of life, which can be normal between outbreaks.
After the operation, and according to the gastroenterologist, will have to continue certain medical treatments to the existing disease in other areas or to prevent their occurrence, as well as continuing review and monitoring. The patient should refrain from smoking. It is interesting to learn more aspects of the disease, patients opinions and expert advice, engage with regional associations of patients with Crohn's disease and ulcerative colitis or national confederation of associations of patients.
Edited by Patricia Crespo Pujante


